
Endometriosis
What is Endometriosis? | Causes of Endometriosis | Symptoms | How is it Diagnosed? | Treatments for Endometriosis
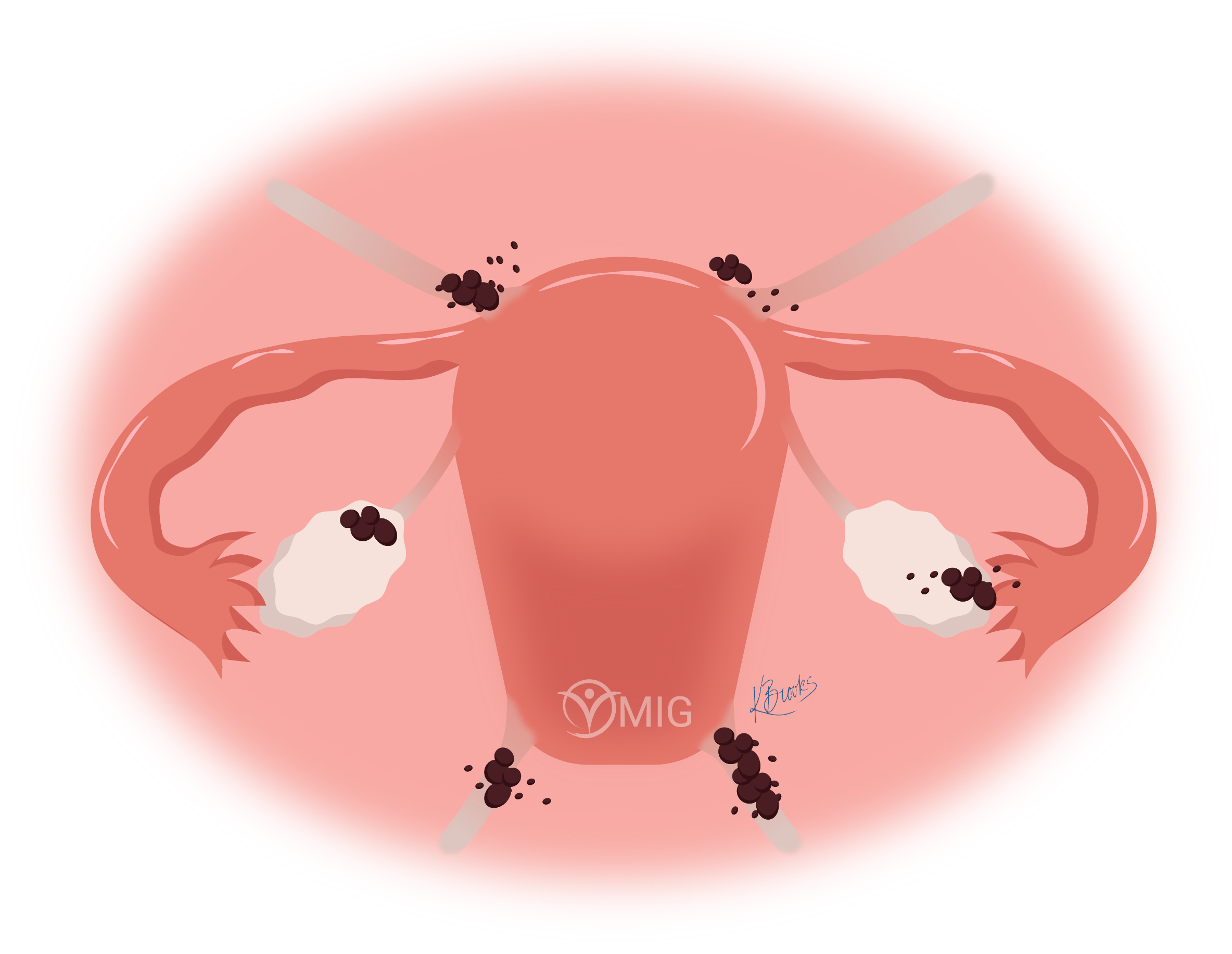
Figure 1. Uterus with endometriosis, including implants, an endometrioma, and an adhesion shown from the front.
The function of endometrial cells is to create a good environment for a fertilized embryo to attach to the uterine wall in the early stages of pregnancy. Hormones produced by the ovaries over the course of the menstrual cycle stimulate the endometrial cells to grow in both size and number, as well as change their function over the cycle. If no pregnancy occurs, the endometrial cells die and are shed, which creates the menstrual flow.
What is Endometriosis?
Endometriosis is a condition where patches of endometrial cells grow outside of the uterine cavity on other organs. This occurs most commonly over the back of the uterus, the ovaries, bladder, and bowels.
The uterus is composed of two main types of cells, muscular and glandular cells. The muscular cells make up the uterine walls and are known as myometrium; while the glandular cells create the lining of the uterine cavity known as the endometrium.
Figure 2. Healthy uterus cross-section shown from the front.
The areas of endometrial tissue outside the uterus (the endometriotic lesions) respond to the ovarian hormones of the menstrual cycle in the same way as the endometrium inside the uterus. Like the endometrium in the womb, the lesions thicken and swell with blood in order to prepare for a possible pregnancy. This swelling causes inflammation which can be painful for the individual.
It is not fully understood why some individuals develop endometriosis and others do not, but there are several theories that explain the condition. The most promising theory is called retrograde menstruation. It is thought that this occurs during menstruation, where small amounts of menstrual blood flow backward through the Fallopian tubes into the abdominal cavity. This blood contains endometrial cells that shed during menstruation. Some of those cells attach and implant onto the pelvic and abdominal cavities and begin to grow and multiply developing into patches or nodules of endometriotic tissue.

Endometriosis is known to run in families. Although a gene that causes endometriosis has not been isolated, a first degree relative (sibling or child) of the individual with endometriosis is seven times more likely to have the condition than someone who does not have a first degree relative with the condition.

Stages of Endometriosis
A system of classification or staging of endometriosis is useful in order to better describe the disease, develop better diagnostic modalities, and treatments as well as to enhance research and standardize communication between scientists and health professionals.
Endometriosis appears in many different forms with a wide variety of clinical presentations depending on the extent of the disease, organs affected, and individual circumstances. Therefore, a classification system for the stages of the disease is not a simple task. The most used and best-known system was developed by the American Society for Reproductive Medicine (ASRM – formerly ASF).
The ASRM classification system is divided into four stages or grades according to the number of lesions and depth of infiltration: minimal (Stage I), mild (Stage II), moderate (Stage III), and severe (Stage IV).
The classification also uses a point system to try to quantify endometriotic lesions. This point system allows for a way to numerically scale the disease. A score of 15 or less indicates minimal or mild disease. A score of 16 or higher may indicate moderate or severe disease. As mentioned before, the severity or score does not necessarily correlate to the level of pain or presence of other symptoms.
ASRM Classification System
Top-down view of the uterus.

Stage I - Minimal (1-5 points)
Few superficial implants

Stage III - Moderate (16-40 points)
Many deep implants
Small cysts on one or both ovaries
Presence of filmy adhesions
Stage II - Mild (6-15 points)
More and deeper implants

Stage IV - Severe (>40 points)
Many deep implants
Large cysts on one or both ovaries
Many dense adhesions
This points system has its limitations and doesn’t always accurately match the patient’s symptoms or likelihood to be able to fall pregnant.
The Endometriosis Foundation of America (Endofound.org) has therefore proposed a different classification using more descriptive categories. It uses the anatomical location and level of infiltration.
ENDOFOUND Endometriosis Classification
Category I: Peritoneal endometriosis
The most minimal form of endometriosis in which the peritoneum, the membrane that lines the abdomen, is infiltrated with endometriosis tissue.
Category II: Ovarian Endometriomas (Chocolate Cysts)
Endometriosis that is already established within the ovaries. These forms of ovarian cysts are of particular concern due to their risk of breaking and spreading endometriosis within the pelvic cavity.
Category III: Deep Infiltrating Endometriosis I (DIE I)
The first form of deep infiltrating endometriosis involves organs within the pelvic cavity. This can include the ovaries, rectum, uterus, and can significantly distort the anatomy of the pelvic organs.
Category IV: Deep Infiltrating Endometriosis II (DIE II)
The other more extreme form of DIE involves organs both within and outside the pelvic cavity. This can include the bowels, appendix, diaphragm, heart and lungs among others.
What is Endometriosis? | Causes of Endometriosis | Symptoms | How is it Diagnosed? | Treatments for Endometriosis